For the 2020 AGM the technical presentations were held digitally via the Zoom platform, and each one was held on a different day. This blog post covers the second, Insights from a large regional HSP cohort, presented by Dr Channa Hewamadduma from Royal Hallamshire Hospital in Sheffield.
HSP
Channa began with a brief introduction to HSP, acknowledging that it is very variable between patients. He described that the SPG genes are numbered in the order of their discovery, and it took a long time to identify the gene for SPG3 and as a consequence this is called At-Last-In or Atlastin!
The spasticity in HSP is due to the degeneration of the motor axons in the spinal cord. He described that, as a parallel, if the diameter of the motor axon were the diameter of a football, then the length of the axon would be 7 football stadia!
Understanding the potential effects of HSP on an individual requires knowing about which type of HSP the person has. In a cohort of HSP patients some will have a family history, but many will not, they are the first person to be affected. The Sheffield cohort has 420 patients, with a clinical dataset for 371 and a gene identified in 211. Of those with a gene identified about 60% are Spast/SPG4 and around a quarter are Paraplegin/SPG7. SPG7 was thought to be rare, but may not be. SPG7 has a later onset. Cerebral palsy has been a common misdiagnosis for younger HSP patients.
Inheritance and Optic Atrophy
More than 40% of patients have bladder involvement and around 40% have pain or spasms. More than half of people with complex HSP have optic atrophy. With optic atrophy problems are spotted when the vision is challenged.
SPG7 is one of the genes which shows the spectra of the different overlaps with other conditions and effects. 10% of those in the Sheffield ataxia clinic have SPG7. SPG7 was discovered in 1998. Sheffield has 55 SPG7 patients, and there is a spread between those with HSP, those with ataxia and those with both. The mean age of onset is 42 years.
Further detail was given on optic atrophy. If people are less able to move their eyes they may have been told they have had a stroke rather than have HSP. Optic atrophy in HSP may mean that people are not able to move their eyes equally in every direction. They are hoping to be able to use this as a biomarker for HSP.
An analysis of published data shows that the age of onset of HSP varies with where the mutation occurs within the gene. If the patient has inherited the same mutation from both parents then their onset may be later than if the patient has inherited different mutations from each parent. If the mutation is sufficient to prevent the protein from working (loss of funciton), the patient would have greater spasticity.
The Sheffield Clinic
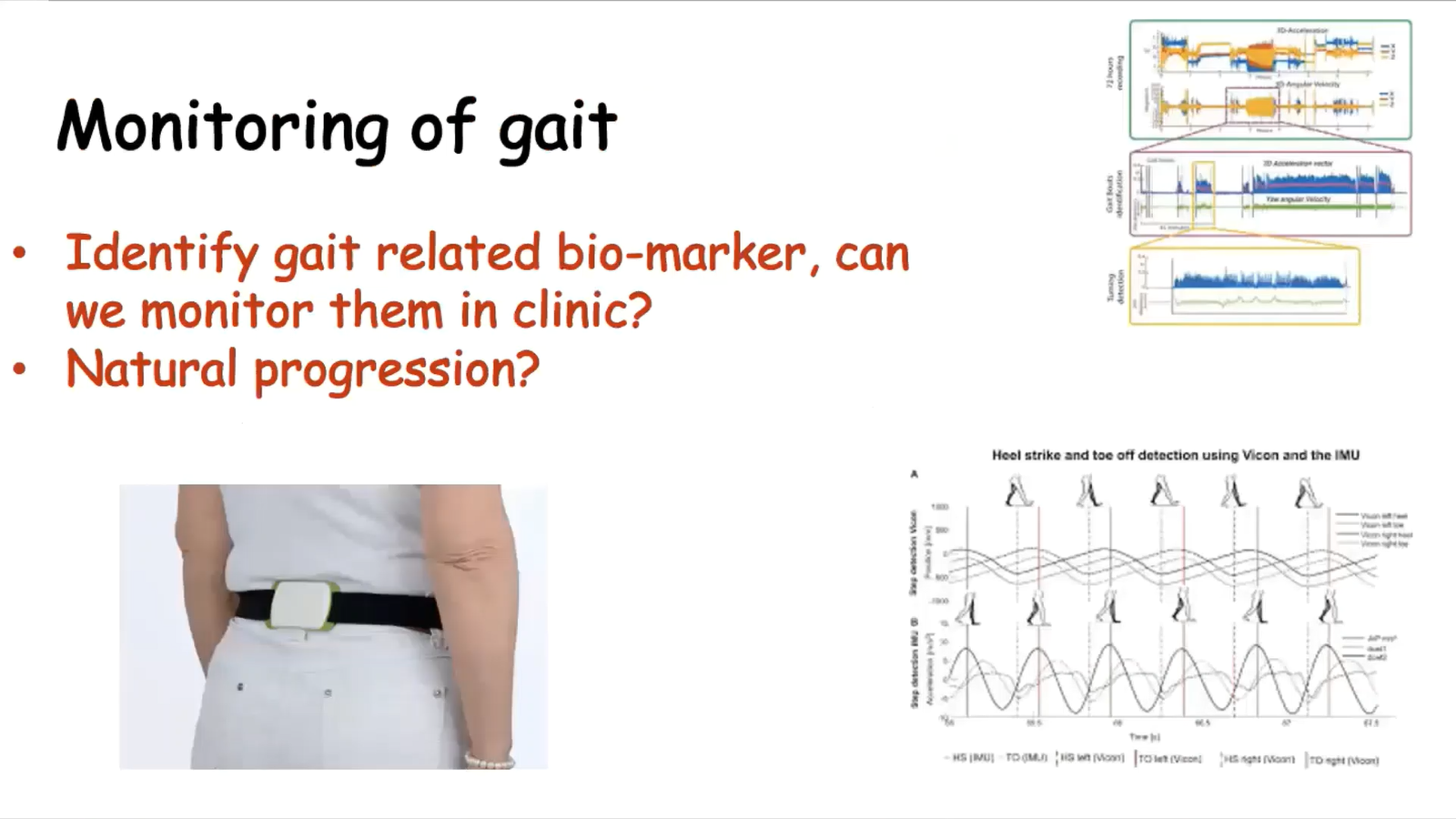
Channa described the in-clinic process for patients, getting an assessment of spasticity, coordination, visual, mood, gait and more. They have a range of interventions available. They are planning to identify the potential for a gait biomarker, to look at the natural progression of HSP and look at the differences between types of HSP.
They have been experimenting with a single sensor gait monitoring, worn on the lower back, which can be used to see how the gait has been affected. Some data was presented looking at a 10m walk test, where a person stands, walks 10m, turns, returns and then sits. Those with SPG4 tend to have more problems standing up, whereas those with SPG7 have more problems sitting down. The gait analysis can also spot effects in mildly affected, which gives them a "trial ready" group of patients.
Future Plans
They are hoping to be able to analyse differences in neuro-imaging to help predict how HSP could progress in an individual.
They are also working on a drug screening programme, looking at the effects of different drugs on cells, from SPG7 , using drugs identified through re-purposing programmes. A high content imaging screen is used to differentiate between cells and controls.
You can watch the whole presentation on YouTube: https://www.youtube.com/watch?v=s3qZqLnNpBY
Q&A
In the Q&A there were a few interesting points.
There is no difference between the terms paraplegia and paraperisis.
There are differences in the mutations in specific types of HSP around the world.
Some people get benefits from co-enzyme Q10, some from CBD oils and some from gluten free diets. A study is planned around the gluten free diet.
For each type of HSP there can be many different mutations. Some of the mutations are more common than others, and there is some variation in the mutation type/location in particular parts of the world.


